
Metformin B12 Deficiency Risk Calculator
Assess Your Vitamin B12 Deficiency Risk
Based on your metformin use and lifestyle factors, this calculator estimates your risk of developing vitamin B12 deficiency. The article explains that 10-30% of long-term users develop deficiency, and risk increases significantly after 5 years.
Your Risk Assessment
Recommended actions: Based on your risk level, consider discussing vitamin B12 testing with your doctor. The article notes that neurological symptoms can appear before blood changes are visible.
For over 25 years, metformin has been the go-to drug for managing type 2 diabetes. It’s affordable, effective, and generally safe. But there’s a hidden risk that many patients - and even some doctors - overlook: long-term use can lead to vitamin B12 deficiency. And when left unchecked, this isn’t just a minor inconvenience. It can cause nerve damage, fatigue, memory problems, and even irreversible spinal cord changes that mimic worsening diabetes.
Here’s the hard truth: if you’ve been on metformin for more than four or five years, your body is likely losing its ability to absorb vitamin B12. It’s not rare. It’s common. Studies show that 10% to 30% of long-term users develop deficiency, and that number jumps to over 50% after 12 years of use. With over 150 million people worldwide taking metformin, millions could be at risk - silently.
How Metformin Steals Your Vitamin B12
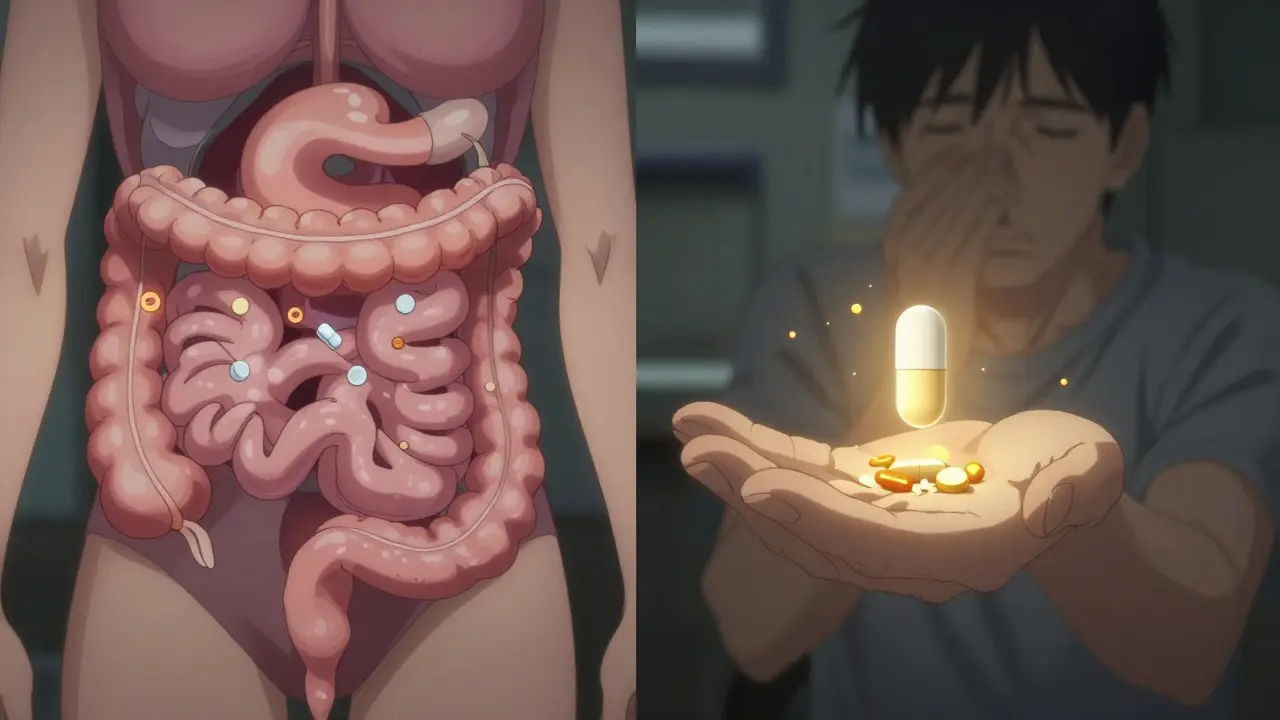
Metformin doesn’t destroy vitamin B12. It blocks its absorption. Here’s how it works: your body needs calcium to absorb B12 from food. In the last part of your small intestine (the ileum), calcium helps attach B12 to special receptors so it can enter your bloodstream. Metformin interferes with this calcium-dependent process. Research from 2023 shows it cuts B12 absorption by 25% to 30%.
It gets worse if you’re also taking proton-pump inhibitors (PPIs) like omeprazole for heartburn. These drugs reduce stomach acid, which is needed to free B12 from food proteins. When you combine metformin and PPIs, the risk of deficiency skyrockets. One study found that 40% of diabetic patients on both drugs had low B12 levels.
And it’s not just about dose - it’s about time. Each extra 1 gram of metformin per day increases your risk of deficiency by more than double. That’s why someone on 2,000 mg daily for 10 years has a much higher chance than someone on 500 mg for two years.
Why Symptoms Are Missed - and Why That’s Dangerous
Here’s the trap: the signs of B12 deficiency look a lot like complications of diabetes.
- Fatigue? That’s common in diabetes.
- Numbness or tingling in hands and feet? That’s diabetic neuropathy.
- Memory lapses or brain fog? Could be high blood sugar.
- Pale or yellow skin? Often blamed on liver issues or anemia from other causes.
But these aren’t just symptoms - they’re red flags. A landmark 13-year study called DPP/DPPOS found that B12 deficiency developed in people on metformin even without anemia. That means your blood count could look normal, but your nerves are already being damaged.
One patient on the NHS forum shared: “After 8 years on metformin, I thought my worsening leg pain was just diabetes. My B12 was 128 pmol/L - normal is above 221. After six months of injections, the numbness faded.”
Another Reddit user described a five-year journey to diagnosis - only to find irreversible spinal cord damage from subacute combined degeneration. That’s not a rare case. It’s preventable.
Who’s at Highest Risk?
Not everyone on metformin will develop B12 deficiency. But some groups are far more vulnerable:
- Long-term users: Anyone on metformin for more than 4-5 years.
- High-dose users: Those taking 2,000 mg or more daily.
- Vegetarians and vegans: They get B12 only from animal products or supplements. No dietary backup means faster depletion.
- PPI users: Acid-reducing drugs make absorption even harder.
- Older adults: Natural decline in stomach acid and B12 absorption compounds the problem.
- People with GI disorders: Crohn’s, celiac, or prior gastric surgery increase risk.
One analysis found that 38% of patients in clinical practice showed neurological symptoms - like balance issues or tingling - before any blood changes appeared. That’s why waiting for anemia to show up is too late.
What Doctors Should Be Doing
Guidelines are changing. In 2022, the UK’s Medicines and Healthcare products Regulatory Agency (MHRA) officially listed B12 deficiency as a common side effect of metformin. The European Association for the Study of Diabetes now recommends checking B12 levels at baseline and every 2-3 years for all patients on metformin.
The American Diabetes Association’s 2024 Standards of Care say: “Periodic measurement of serum B12 levels should be considered, especially in those with anemia or neuropathy.”
But here’s the gap: many GPs still don’t test unless anemia is present. That’s outdated. You don’t need low hemoglobin to have nerve damage. The real test is not just B12 levels - it’s methylmalonic acid (MMA) and homocysteine. These are functional markers that show if your cells are truly starved of B12, even when serum levels look borderline.
What You Can Do - Right Now
If you’ve been on metformin for years, here’s what to ask your doctor:
- “Can you test my vitamin B12 level?” Request a serum B12 test. Normal is typically above 221 pmol/L (or 300 pg/mL).
- “Should I also get MMA and homocysteine checked?” These are more accurate indicators of tissue deficiency.
- “Am I in a high-risk group?” If you’re vegetarian, on PPIs, or over 60, push for testing even if you feel fine.
If your levels are low, treatment is simple:
- High-dose oral B12: 1,000-2,000 mcg daily. Surprisingly, this works well even for absorption issues.
- Injections: 1,000 mcg weekly for 4 weeks, then monthly. Best for severe deficiency or neurological symptoms.
One study found that 89% of patients improved hematologically within three months of starting supplements. Nerve symptoms often take longer - up to 6-12 months - but many patients report dramatic improvements in energy, balance, and numbness.
A Surprising Prevention Trick
There’s a simple, low-cost way to reduce your risk: calcium.
A 2021 randomized trial in Diabetes Care gave 1,200 mg of calcium carbonate daily to metformin users. After two years, those taking calcium had a 47% lower risk of B12 deficiency. Why? Calcium helps restore the receptor function that metformin disrupts. It’s not a cure, but it’s a powerful shield.
You don’t need a prescription. Over-the-counter calcium supplements (like Tums or generic calcium carbonate) can help. Talk to your doctor about adding 1,200 mg daily - especially if you’re on high-dose metformin.
The Bigger Picture
This isn’t just about one drug. It’s about how we manage chronic conditions. We focus so hard on blood sugar that we forget the body needs more than insulin control. Nutrient gaps accumulate over years. And when they do, the damage can be permanent.
By 2025, experts predict that routine B12 testing will be standard in all major diabetes care programs. The cost? Around $18-25 per patient per year. The savings? Up to $187 per patient in prevented complications - from nerve clinics to hospital admissions for falls and misdiagnosed neuropathy.
And research is moving forward. A 2023 study identified genetic variants in the cubilin receptor gene (CUBN) that make some people far more susceptible. In the future, we may screen for these before prescribing metformin.
For now, the message is clear: if you’ve been on metformin for years, don’t wait for symptoms. Ask for a B12 test. Ask about calcium. Don’t assume your fatigue or numbness is just diabetes. It might be something far simpler - and far easier - to fix.




13 Comments
Jimmy V
March 13, 2026Metformin users, listen up. This isn't hype - it's biochemistry. If you've been on it for 5+ years, your B12 is probably tanking. No anemia? Doesn't matter. Nerve damage doesn't wait for your CBC to look 'normal.' Get MMA and homocysteine tested. Not just serum B12. And yes - calcium supplements help. 1200mg daily. Tums works. Stop ignoring this.
Byron Boror
March 15, 2026Another reason to ditch the diabetes-industrial complex. Big Pharma doesn't want you knowing metformin slowly fries your nerves. They profit off the complications - nerve clinics, fall treatments, endless lab tests. Meanwhile, a $5 calcium pill could've saved you from lifelong disability. Wake up.
Kandace Bennett
March 16, 2026OMG YES. I'm a vegan on metformin and I thought my brain fog was just 'adulting.' Turns out my B12 was 140. 😱 Six months of injections and I'm basically a new person. Energy? Like I drank 5 espressos. Numbness? Gone. You're not 'just tired' - you're deficient. Go get tested. Now. 💉✨
Lorna Brown
March 17, 2026What's fascinating here isn't just the mechanism - it's how medicine ignores systemic nutrient depletion in chronic disease management. We treat blood sugar like it's the only variable in the equation. But the body is a network, not a dashboard. Deplete B12, and you don't just get numb feet - you disrupt methylation, homocysteine metabolism, myelin synthesis. This isn't a side effect. It's a cascade. And we're failing patients by treating symptoms, not root causes.
Richard Harris
March 18, 2026Interesting read. I've been on metformin for 7 years. Never thought about B12. My doc never mentioned it. Might get it checked next time I'm in. Thanks for the nudge. 🙏
Dylan Patrick
March 19, 2026Bro. I'm a nurse. I've seen this. Patient comes in with 'diabetic neuropathy' - numb toes, balance issues. We run labs. B12 at 110. Give 'em shots. Two months later? They're walking without a cane. No magic. Just basic science. Stop overcomplicating it. Test. Supplement. Fix it. Simple.
Rex Regum
March 21, 2026So let me get this straight - we're blaming a life-saving drug for 'stealing' a vitamin? What's next? Is insulin causing zinc deficiency? Are we going to start telling people with hypertension to eat more potassium because they're 'deficient'? This is fearmongering dressed as science. If you're worried about B12, take a supplement. Don't panic over a 30-year-old drug that's saved millions from amputations.
Jinesh Jain
March 22, 2026Interesting. I'm from India, on metformin 10 years. No symptoms. But I eat eggs, milk, yogurt daily. Maybe diet matters. I'll ask my doctor about MMA test. Not sure if it's available here.
Noluthando Devour Mamabolo
March 24, 2026Per the 2023 ICD-11-aligned clinical guidelines, the subclinical B12 deficiency cascade in metformin-exposed cohorts is mediated by CUBN receptor downregulation, compounded by PPI-induced achlorhydria. Functional biomarkers (MMA >0.4 µmol/L, homocysteine >12 µmol/L) are more predictive than serum B12 thresholds. Prophylactic calcium carbonate (1200mg/day) demonstrates NNT of 4.3 to prevent deficiency. Recommend tiered screening per risk stratification.
mir yasir
March 25, 2026It is indeed a matter of grave concern that the medical community has not yet universally adopted the practice of routine B12 monitoring in patients undergoing prolonged metformin therapy. The evidence base is robust, and the cost-benefit ratio is overwhelmingly favorable. One must question the inertia within primary care protocols in the face of such preventable morbidity.
Stephanie Paluch
March 25, 2026my mom had this. thought it was just aging. then she got the injections and suddenly she could walk without holding the wall. i cried. if you're on metformin - just get tested. it's so easy. please.
Leah Dobbin
March 26, 2026I'm surprised this isn't common knowledge yet. Honestly, if you're on metformin for more than a few years and haven't thought about B12, you're not being proactive - you're just lucky. And luck isn't a medical strategy.
tynece roberts
March 28, 2026so i've been on metformin since 2018 and i'm vegan and i take omeprazole and i've been super tired and my feet feel like they're wrapped in saran wrap? i just thought i was getting older. i'm gonna go get my b12 checked like rn. also i think i'm gonna start taking tums with meals? lol. thanks for the heads up. i feel dumb but also so relieved.