
When you have COPD, your lungs aren’t the only thing suffering. Many people don’t realize that sarcopenia - the loss of muscle mass and strength - is one of the most dangerous complications of the disease. It’s not just about getting older. In COPD, muscle wasting happens faster, hits harder, and steals your ability to breathe, walk, or even get out of bed. About 1 in 5 people with COPD have sarcopenia, and those who do are 20-40% more likely to die within five years than those who don’t. The good news? You can fight it. Not with a pill, but with food and movement - the right way.
Why Sarcopenia Hits Harder in COPD
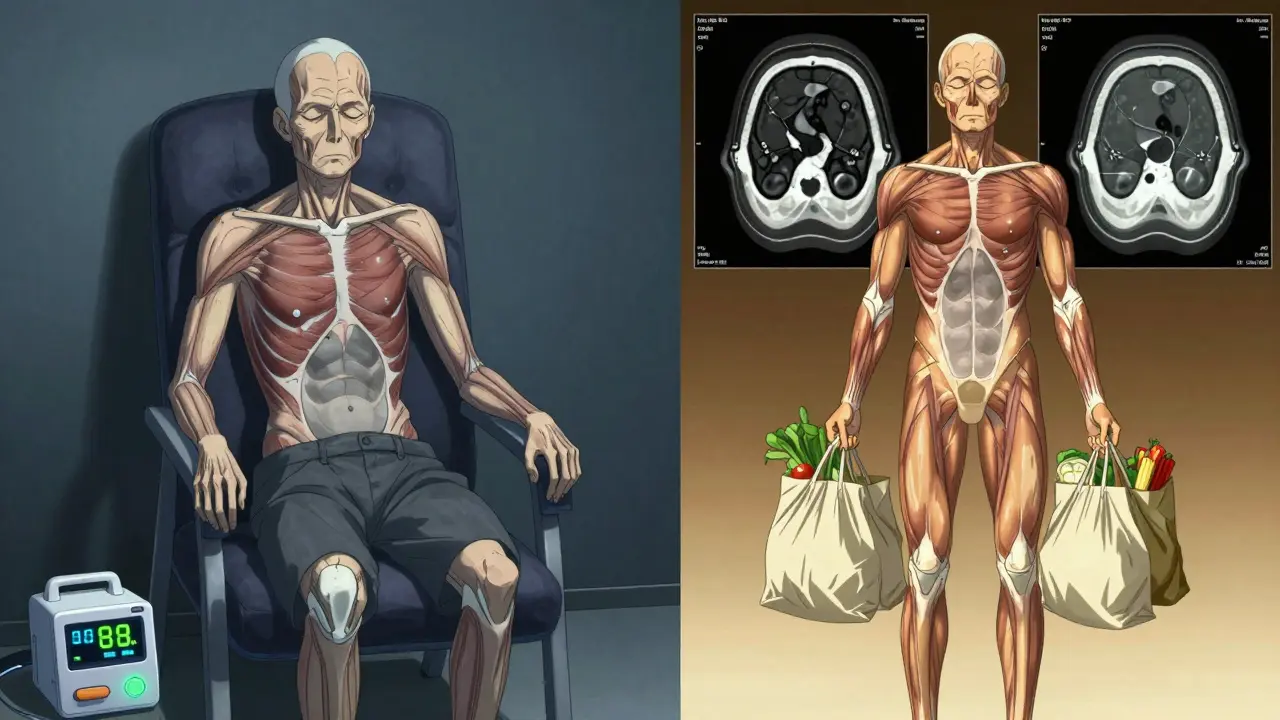
Most people think muscle loss just comes with age. But in COPD, it’s worse. Your body is stuck in a cycle: low oxygen, inflammation, and inactivity all team up to break down muscle faster than normal aging. Studies show people with COPD lose muscle at 3.2% per year - double the rate of healthy older adults. And it’s not just your legs. Your breathing muscles - the diaphragm, the chest muscles - start shrinking too. That’s why even simple tasks like lifting a bag of groceries or climbing stairs become impossible.One key clue? Your pectoralis muscle. That’s the big chest muscle you use when you breathe deeply. In COPD patients with sarcopenia, it’s often 68% thinner than in people without COPD. CT scans show this clearly. And here’s the scary part: if your oxygen levels drop below 88% for more than 30% of the night, your risk of severe muscle loss jumps by 47%. Sleep isn’t rest - it’s another battlefront.
How to Know If You Have It
Doctors used to miss sarcopenia because they focused only on lung function. Now, guidelines say every COPD patient should be screened. The easiest way? Handgrip strength. If you’re a man and your grip is under 27 kg (about 60 lbs), or a woman under 16 kg (35 lbs), that’s a red flag. But that’s just step one.Next, check your movement. Can you walk 4 meters in under 0.8 seconds? Can you stand up from a chair five times without using your hands? If not, your physical performance is declining. These are part of the Short Physical Performance Battery (SPPB), now used in clinics worldwide. Some hospitals also use DEXA scans to measure muscle mass in your arms and legs. But you don’t need a scan to start acting. If you’re weaker than you were a year ago, or you’re getting breathless doing less, sarcopenia might be part of the problem.
What Nutrition Really Looks Like
Most COPD patients eat too little protein. On average, they get only 0.9 grams per kilogram of body weight. The science says you need 1.2 to 1.5 grams. That’s not a suggestion - it’s a requirement. For a 70 kg (154 lb) person, that’s 84 to 105 grams of protein a day. Think: three eggs at breakfast, a chicken breast at lunch, a cup of Greek yogurt with nuts at snack, and a salmon fillet at dinner.But it’s not just about quantity. Timing matters. Your muscles can only use so much protein at once. Spreading it out over 4 meals - with 25-30 grams per meal - keeps muscle building active all day. One study found that adding 2.5 to 3 grams of leucine per meal (found in whey protein, eggs, and meat) boosts muscle synthesis by 37%. That’s why many doctors now recommend a whey protein shake with leucine after meals, especially if appetite is low.
Don’t forget calories. Many COPD patients burn 20-30% more energy just breathing. If you’re not eating enough, your body starts using muscle for fuel. A dietitian can help you find calorie-dense, easy-to-eat foods: nut butters, full-fat dairy, smoothies with protein powder, avocado, and olive oil. You don’t need to eat huge meals - just eat more often.
Resistance Training That Actually Works
You’ve probably heard: “Exercise helps.” But for someone with COPD, traditional gym routines can make breathing worse. That’s why standard programs fail. The key is starting low and going slow.Begin with 30% of your one-rep maximum - that’s the most weight you could lift once. For most people, that means 1- to 2-pound dumbbells or resistance bands. Do 10-12 reps of exercises like seated shoulder presses, leg extensions, and seated rows. Two to three times a week. Rest 2-3 minutes between sets. If you feel dizzy or too short of breath, stop. Don’t push through.
Progress is slow. It takes 8-12 weeks to see real strength gains. But the payoff? A 23% improvement in how far you can walk in 6 minutes. That’s not just a number - it’s being able to walk to the mailbox without stopping. Or standing while cooking. Or playing with your grandkids.
Here’s what works: Supervised pulmonary rehab programs. These are not generic gyms. They’re designed for COPD. Trainers know how to adjust for oxygen needs. Many patients need supplemental oxygen during training - 42% do. If your program doesn’t offer that, ask for it. Or find one that does.
What to Avoid
Many patients quit because they were told to “just lift weights” without guidance. That’s dangerous. Heavy lifting, holding your breath, or doing too much too soon can spike your heart rate and oxygen demand, triggering a flare-up. Avoid:- Exercises that require holding your breath (like heavy squats or planks)
- High-intensity interval training (HIIT) without supervision
- Skipping oxygen during exercise
- Waiting until you feel weak to start
Also, don’t rely on protein bars or shakes that don’t list leucine content. Many are full of sugar and fillers. Look for whey isolate with at least 2.5 grams of leucine per serving. If you’re unsure, ask your dietitian.
Real Stories, Real Results
Mary, 68, had GOLD Stage 3 COPD. She couldn’t carry her purse without stopping to catch her breath. After 12 weeks of a pulmonary rehab program with light resistance bands and protein shakes, she could walk to the store and carry two bags home. “I didn’t know muscle loss was part of COPD,” she said. “Now I feel like myself again.”John, 72, tried resistance training at home. He didn’t use oxygen. He got so breathless he quit after three sessions. “I thought I was being strong,” he admitted. “I was just hurting myself.”
At the Cleveland Clinic, 78 patients followed a 16-week plan: protein (1.2 g/kg/day) + supervised resistance training. Their walking distance improved by 23%. Hospital stays dropped. Quality of life rose. This isn’t theory. It’s happening.
What’s Next
New research is coming fast. The Global Initiative for Chronic Obstructive Lung Disease (GOLD) just released its first sarcopenia management algorithm - tying nighttime oxygen levels to exercise prescriptions. A major European trial is testing HMB, a supplement that helps preserve muscle, combined with training. And a new drug targeting myostatin (a protein that limits muscle growth) is in phase 2 trials, with results expected in 2025.But you don’t have to wait. The tools are here now. Screen yourself. Talk to your doctor. Ask about a pulmonary rehab program. Ask about protein. Ask about oxygen during exercise. You don’t need to be perfect. You just need to start.
Is sarcopenia the same as general muscle loss in older adults?
No. While both involve muscle loss, sarcopenia in COPD is more aggressive and affects different muscles. In healthy aging, leg muscles decline first. In COPD, the chest and breathing muscles are hit hardest. Muscle loss also happens faster - 3.2% per year versus 1-2% in healthy aging. Inflammation and low oxygen levels from COPD accelerate the process in ways that normal aging doesn’t.
Can I do resistance training at home without a gym?
Yes - and it’s often safer. Start with resistance bands or light dumbbells (1-2 lbs). Do seated exercises: shoulder presses, leg extensions, seated rows. Use a chair for support. Do 10-12 reps, 2-3 times a week. Rest 2-3 minutes between sets. If you feel dizzy or too breathless, stop. You don’t need equipment - bodyweight squats against a wall or heel raises while holding a counter work too. The goal is consistency, not intensity.
How much protein should I really be eating?
You need 1.2 to 1.5 grams of protein per kilogram of body weight daily. For a 70 kg (154 lb) person, that’s 84-105 grams. Spread it over 4 meals - about 25-30 grams per meal. A 3-ounce chicken breast has 26g. One cup of Greek yogurt has 17g. Two eggs have 12g. Add a whey protein shake with 10g leucine after one meal. Most COPD patients eat only 0.8-1.0 g/kg - far below what’s needed to rebuild muscle.
Do I need oxygen during exercise?
Many do - 42% of COPD patients need supplemental oxygen during resistance training. If you’re on oxygen at rest, you likely need it during activity too. Ask your doctor for an exercise oxygen test. If you get short of breath while lifting light weights, don’t push through. Use your oxygen. It’s not a sign of weakness - it’s a tool to help you get stronger safely.
What if I can’t afford pulmonary rehab?
Many community centers, libraries, or senior centers offer low-cost or free pulmonary rehab programs. Medicare and some private insurers cover them if prescribed by a doctor. If cost is an issue, start with home-based exercises and protein. Use free online videos designed for COPD (look for ones from the American Lung Association or COPD Foundation). Track your progress: can you stand up from a chair faster? Walk farther? That’s your win.
Can sarcopenia be reversed in advanced COPD?
Yes - even in advanced stages. Studies show patients with GOLD Stage 3 and 4 COPD improve strength and walking distance with consistent nutrition and training. It takes longer - often 16-24 weeks - but gains are real. The key is starting before you’re too weak. If you’re already struggling to get out of bed, talk to your doctor about starting with seated exercises and protein shakes. Every bit of muscle you rebuild improves your breathing, your stamina, and your chances of living longer.

15 Comments
Johny Prayogi
March 20, 2026This is the most practical, no-BS guide to fighting sarcopenia I've ever read. Seriously, 1.2-1.5g/kg protein? I was eating 0.8g/kg and wondering why I couldn't lift my cat. Started hitting 105g/day with Greek yogurt, eggs, and a whey shake after breakfast. Three weeks in - I can now carry my laundry basket without gasping. Game changer.
Desiree LaPointe
March 21, 2026Oh wow. Another medical miracle delivered via protein shakes and light dumbbells. How quaint. The pharmaceutical industry must be weeping. Next you'll tell us sunlight cures depression and water hydrates you.
Meanwhile, in the real world, 42% of COPD patients need supplemental oxygen during exercise - and yet we're being told to 'just lift 1-lb weights' like we're in a geriatric yoga class. Where's the funding? Where's the innovation? This is band-aid medicine dressed up as a revolution.
Paul Cuccurullo
March 22, 2026I'm not a doctor, but I've been living with COPD for 11 years. I started this regimen six months ago. Protein. Light bands. Oxygen during training. I went from 270 feet in 6 minutes to 580. I can hug my grandkids again. Not because of magic. Not because of pills. Because someone finally said: 'Your body is still worth fighting for.'
Nicole James
March 23, 2026I’ve been waiting for this. The government, the AMA, Big Pharma - they’ve all been hiding the truth. Sarcopenia isn’t just muscle loss. It’s a symptom. A symptom of systemic oxygen deprivation. And oxygen deprivation? That’s caused by… *checks notes*… corporate pollution policies. The real villain isn’t your diaphragm. It’s the coal plants. The oil lobbies. The FDA’s silence. We’re being slowly suffocated - and then told to eat more eggs. 🤔
Sandy Wells
March 24, 2026I read this and thought - this is exactly what my pulmonologist skipped over. I’ve been on oxygen 24/7 since 2020. Never once was I told to track my protein intake or do seated rows. I’m 65. I’ve been told to rest. To slow down. To accept decline. This article says: fight. And I’m starting tomorrow.
Shaun Wakashige
March 25, 2026Meh. I tried the protein shake thing. Tasted like chalk. Gave up after 3 days. Still can’t lift my dog. Guess I’m just gonna die slowly. 🤷♂️
Chris Dwyer
March 27, 2026If you're reading this and thinking 'I'm too weak to start' - I get it. I was there. I used to cry after climbing one flight of stairs. But here's the thing: you don't need to be strong to begin. You just need to show up. One band. One egg. One minute of movement. That's your victory. Keep showing up. I promise - your body remembers you care.
Jackie Tucker
March 27, 2026Ah yes. The classic 'nutrition and light weights' solution. So elegant. So... bourgeois.
Let me guess - this advice is meant for those with access to whey isolate, a quiet kitchen, and a therapist to help them cope with the trauma of being told they're 'not trying hard enough'. Meanwhile, the 70-year-old on fixed income, living in a food desert, with no transportation to rehab?
Good luck with that.
Thomas Jensen
March 28, 2026I don't trust this. They say 'supervised rehab' works. But who supervises the supervisors? What if they're just pushing this because the equipment manufacturers are funding the studies? What if the oxygen masks are overpriced? What if the leucine is laced with something? I read a forum post once that said 68% of pulmonary rehab centers have hidden cameras. I don't know. I just feel watched.
matthew runcie
March 29, 2026I’ve been doing this for 4 months. No dramatic results. But I can now get up from the couch without needing a nap. That’s something. I’m not trying to run a marathon. Just to not be a burden. This isn’t a cure. It’s a pause in the fall. And I’ll take it.
shannon kozee
March 31, 2026Handgrip strength under 27kg = red flag. My husband’s is 24. We started protein shakes last week. He’s sleeping better. Not because of the shakes. Because he’s trying. That’s the real win.
trudale hampton
April 1, 2026I’ve been doing seated resistance bands for 3 weeks. No gym. No oxygen yet. Just me, a chair, and a YouTube video from the COPD Foundation. I can now open a jar without crying. That’s progress. Slow. Quiet. Real.
Solomon Kindie
April 2, 2026So the solution to muscle wasting is more protein and more movement? Wow. Groundbreaking. Next you’ll tell us gravity is real and the earth is round. Why not just inject us with muscle? Why not gene edit our myostatin? Why are we still stuck in the 1990s with dumbbells and yogurt? This is like telling a cancer patient to eat more kale and hope for the best.
Natali Shevchenko
April 4, 2026There’s a deeper layer here, you know. Sarcopenia in COPD isn’t just physiological. It’s existential. Every time you can’t lift your coffee cup, you’re reminded: your body is betraying you. And society? It tells you to rest. To accept. To fade. But what if resistance - literal, physical resistance - is also a spiritual act? Each rep, each gram of protein, each breath with oxygen - it’s not just about strength. It’s about saying: I am still here. I still choose to be. Even if I’m broken. Even if I’m tired. Even if I’m 72. I choose to fight. Not for a longer life. But for a life that still feels like mine.
Nishan Basnet
April 5, 2026This is beautiful. I work with elderly COPD patients in Delhi. Many can’t afford protein powder. So we use lentils, eggs, and milk - boiled with turmeric. One man, 78, couldn’t stand without help. Now, after 14 weeks of seated resistance with a water bottle and 3 eggs a day? He walks to the temple every morning. No fancy gear. Just consistency. And community. This works anywhere. If you care.